
The shoulder girdle consists of three bones, the humerus (arm bone), scapular (shoulder blade) and clavicle (collar bone) articulating with the chest wall. The movement of the shoulder occurs between the scapular and the chest wall and at the true shoulder joint (glenohumeral joint) itself. The clavicle is a strut and provides a bony connection between the shoulder and the remainder of the skeleton.
|
The shoulder joint is a ball and socket joint that allows a high degree of mobility to enable the positioning of our hands and upper limb in order to manipulate our environment.
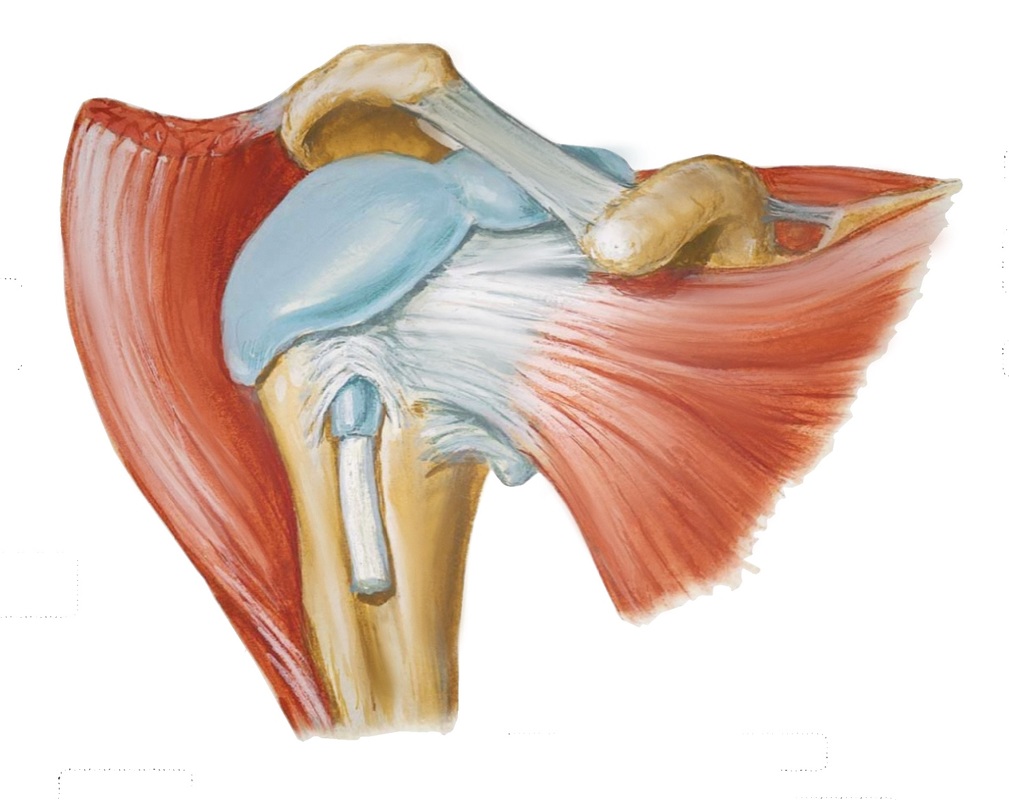
To allow for a large range of motion, the bony anatomy is one of a shallow socket and a large ball (Similar to a golf ball on a tee). Stability relies heavily on the the soft tissues (muscle, tendon and ligaments) around the joint. The glenoid (socket) is deepened by cartilage and a surrounding ligament (the labrum). The capsule and associated ligaments and muscle help to stabilise the joint even further.
To allow for a large range of motion, the bony anatomy is one of a shallow socket and a large ball (Similar to a golf ball on a tee). Stability relies heavily on the the soft tissues (muscle, tendon and ligaments) around the joint. The glenoid (socket) is deepened by cartilage and a surrounding ligament (the labrum). The capsule and associated ligaments and muscle help to stabilise the joint even further.
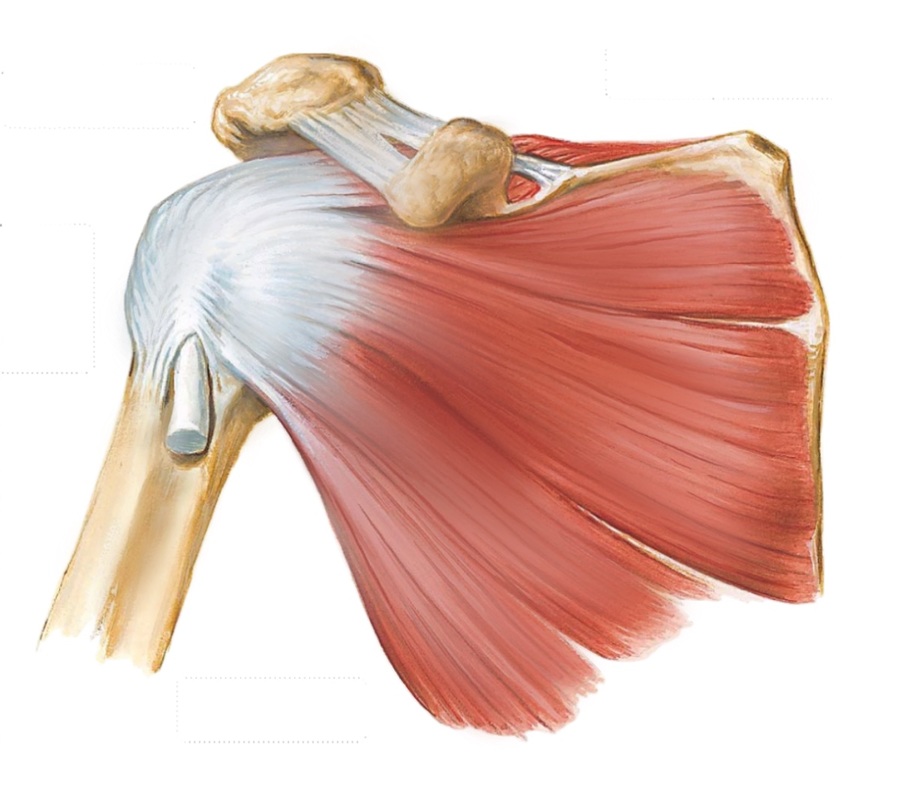
There are two layers of muscle that stabilise and move the shoulder joint. The inner layer of muscle is called the rotator cuff and the outer layer of muscle includes the Deltoid and Pectorals Major (Pectoral muscle). The role of the rotator cuff muscles are to keep the humeral head centred over the glenoid socket as well as to rotate the humeral head within the glenoid socket for accurate positioning of the shoulder joint. The outer layer of muscles provide power and leverage to the shoulder.
The inner and outer layer of muscle slide over each other and slide in different directions with shoulder movement. This can create friction. To reduce friction, a fluid filled sac called the subdeltoid bursa is found between the outer and inner layer of muscles. Unfortunately the subdeltoid bursa itself can become irritated and inflamed and is a common cause of shoulder pain and loss of function.
The inner and outer layer of muscle slide over each other and slide in different directions with shoulder movement. This can create friction. To reduce friction, a fluid filled sac called the subdeltoid bursa is found between the outer and inner layer of muscles. Unfortunately the subdeltoid bursa itself can become irritated and inflamed and is a common cause of shoulder pain and loss of function.
|
Conditions affecting the shoulder
Soft tissue conditions of the shoulderFailure of the soft tissue structures around the shoulder joint are common conditions affecting the shoulder. This can be due to an injury or wear and tear as the result of age and/or repetitive activities. This can lead to pain, weakness or instability and ultimately can affect the function of the shoulder.
Common soft tissue condition affecting the shoulder include the following.
Arthritis of the shoulder.Arthritis is the wearing down of the lining cartilage of a joint and it can affect the shoulder joint like any other joint in the body.
This leads to pain and stiffness and is not reversible. In the shoulder the arthritis can be a primary age related process (osteoarthritis), a result of trauma or a systemic inflammatory disease ( such as rheumatoid arthritis). It can also be a consequence of untreated failure of the soft tissues. If the rotator cuff is torn, this can lead rotator cuff muscle imbalance and loss of the ability to keep the humeral head centred over the glenoid. This results in arthritis of the shoulder (a condition called cuff tear arthropathy), Arthritis can also occur with untreated shoulder instability due to a labral tear. Repeated dislocations of the shoulder can lead to the damage of cartilage Arthritis can also affect the accessory joints around the shoulder such as the acromioclavicular joint ( AC Joint ) and less commonly, the Sternoclavicular joint ( SC Joint ). |
Fractures around the shouldeerFractures around the shoulder joint are complex injuries. Proximal humerus fractures can occur in the elderly with a simple fall or in young patients with high energy trauma. Although a large proportion of these can be treated with simple immobilisation. Some displaced fractures require surgery due to the significant pull from the muscles attached to the fractured fragments.
Scapular and glenoid fractures are a result of significant trauma such as a road traffic accident or a fall from height. The ultimate goal of treatment for these injuries is to restore anatomical relationships of the structures in order to preserve the normal biomechanics of the shoulder joint. Clavicle (Collarbone) fractures can cause patients' a lot of distress. In deciding the treatment for these injuries, a consideration is made based on the patient and the fracture characteristics. It is important to maintain the length of the clavicle in order maintain the 'offset' of the shoulder. Dislocations around shoulderShoulder dislocations can occur from contact sports, a fall or motor vehicle trauma. It can lead to recurrent instability due to a tearing of the labrum as well as fracture of part of the glenoid ( socket ) bone that fails to heal (Bony Bankart lesion). As the humeral head dislocates out of the joint, the edge of the glenoid often causes an impaction in the bone of the humeral head (a Hill Sachs lesion). If large enough this can repeatedly catch on the edge of the glenoid as the humeral head rotates and cause the shoulder to dislocate (engaging Hill Sachs lesion).
Acromioclavicular joint dislocations often occur as a result of a fall (often off a push bike). The outer end of the clavicle dislocates from the acromioclavicular joint due to stretching or a complete tear of the ligaments that tether the clavicle to the coracoid process of the scapular (coracoclavicular ligaments). Dislocations that are of a higher grade where there is no contact between the outer end of the clavicle and the acromion at the AC joint should be considered for surgery. This is particularly true for younger patients or patients with high functional demands on their shoulder. |
Shoulder surgery
|
Shoulder surgery is a highly specialised field of orthopaedic surgery. Most orthopaedic surgeons in Australia have limited exposure to shoulder surgery through their formal orthopaedic surgery training. Knowledge and expertise with the conditions affecting the shoulder and the extensive treatments (both surgical and non surgical) is often gained with additional subspecialty training.
Arthroscopic surgery, a revolution in shoulder surgeryDue to the deltoid muscle covering the shoulder joint and the intimate relationship between the rotator cuff muscles and the shoulder joint capsule, traditional open surgery of the shoulder has required detachment of these muscles in order to access the joint. This in itself has caused well recognised morbidity due to failure of the detached muscle to heal. Open surgical wounds are large and can cause a significant amount of pain in the recovery period.
The advent of arthroscopic surgery of the shoulder has enabled a minimally invasive and muscle sparring approach to the shoulder without the need to detach the deltoid or the rotator cuff muscles (usually subscapularis muscle) to gain full access to the shoulder joint. In addition, an arthroscopic surgeon can visualise the all aspects of the shoulder joint in great detail to diagnose and treat associated conditions that may be missed during an open procedure where the field of view is only the portion of the shoulder exposed by the surgical incision. Additional benefits of arthroscopic surgery include less post surgical pain and a faster recovery. Although the size of the surgical wound should not be a primary consideration for orthopaedic surgery, many patients prefer a smaller scar. Shoulder arthroscopy requires highly specialised equipment and the mastery of shoulder arthroscopy requires a steep learning curve on the part of the surgeon. However, shoulder arthroscopy has allowed procedures that have been traditionally performed by open surgery to be performed arthroscopically. This includes following procedures.
|
Open shoulder surgery remains relevantOpen shoulder surgery still remains relevant in shoulder surgery and many shoulder procedures that are performed by open surgery are still considered to be the gold standard (yardstick) by which the success of other techniques are measured.
Many surgeons perform rotator cuff repair surgery through an open or mini open incision with very successful outcomes. This approach is reliable and less complex than an arthroscopic rotator cuff repair. Many operations require an open approach as the techniques and technology has not allowed a less invasive approach. This includes treatment of fractures, ligament reconstructions, tendon transfers and repairs and shoulder replacement procedures. Shoulder arthroplastyShoulder replacement surgery is used to treat patients who have end stage arthritis of the shoulder, shoulder fractures and for patients with large rotator cuff tears that can't be repaired.
The different types of shoulder replacements include shoulder resurfacing, hemi-arthroplasty (replacing only the humerus), total anatomical shoulder replacement and reverse shoulder replacement. The most common shoulder replacements performed in Australia is the reverse followed by anatomical total shoulder replacement. The reverse shoulder replacement reverses the ball and socket so that an articulating sphere (glenosphere) is placed at the native Glenoid and the humeral head is altered to create an articulating socket for the glenosphere. 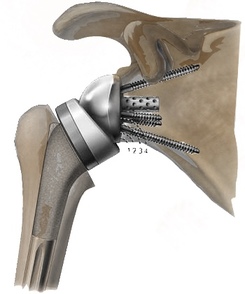
A reverse shoulder replacement is performed for cuff tear arthropathy, rotator cuff tears that are not repairable, fractures of the proximal humerus and for revision of a failed previous shoulder replacement.
An anatomical total shoulder replacement is used for primary osteoarthritis where the rotator cuff is not torn. Shoulder replacements are generally not as durable as replacements of the hip and knee. The reasons for this are attributed to shoulder arthroplasty being less commonly performed. Shoulder replacement prosthesis are also not as good at restoring the complex anatomy or biomechanics of the shoulder joint. With refinements in implants and surgical technique, outcomes have improved over the past 10 years and it is likely that this improvement will continue going forward. |